

I just got back from San Diego and wanted to share something that I think is going to be very popular among orthodontists who are serious about delivering quality care and doing things the right way. In a meeting with an overseas orthodontic company, I was given this reprint of a paper that is about to come out. The authors, Dr. Swift and Clemens, have very exclusive practices, are known for their high-quality treatment and they service the who’s who of Europe. They have used and studied bonded retainers extensively and have come to some conclusions that may force a paradigm shift in retention. Welcome to Ortho 2.0…
Risk of complications between maxillary palatal fixed retainers and maxillary labial fixed retainers: A clinical study.
Swift, J, Clemens, S.
Introduction
Patient compliance with removable retainers will determine the longevity of their ideal orthodontic treatment result.1 Even though patients are educated about the need for prolonged retention after treatment and asked to sign an informed consent regarding the risk of relapse; many orthodontists would estimate that at least half of their teenage patients do not comply at optimal levels. In the past 30 years, the fixed retainer has supplanted the use of the removable retainer.2 Many orthodontists have been resistant to using fixed retainers because they feel that these retainers are more prone to complications with regard to breakage, more technique sensitivity, and the patient’s inability to maintain proper oral hygiene.3 The aim of the present study was to compare the risk of complications between traditional maxillary palatal fixed retainers in comparison to maxillary labial fixed retainers.
Materials and Methods
Power calculations were used to determine the appropriate sample size to detect statistical differences between groups. The final study sample consisted of 30 subjects in the labial fixed retainer test group (12 males and 18 females, mean age 14.6 years) and 30 subjects in the palatal fixed retainer control group (17 males and 13 females, mean age 14.2 years). The inclusion criteria for both groups were matching by age and gender, non-extraction orthodontic treatment of at least moderate crowding, and no missing anterior teeth. Four different types of maxillary labial fixed retainers were used and were randomly allocated to the test subjects (Figs.1-4). A standard type of maxillary palatal fixed retainer was used for the entire control group (Fig. 5). All types of retainers were bonded via the acid etch technique with a light cure bond enhancer and a light cured adhesive. The fixed retainers were all placed on the day of debond. The fixed retainers were checked at a 6 month follow up appointment. Complications were defined as: broken bond(s), broken wire, or poor gingival health.
Results
The occurrence of complications in the test and control groups were grouped and summarized in Table 1. The risk of complications in the entire sample (17/60)*100 was 28%. The risk of complications in the maxillary labial fixed retainer test group (3/30)*100 was 10%. The risk of complications in the maxillary palatal fixed retainer control group (14/30)*100 was 47%. While the risk of having complications in the maxillary labial fixed retainer test group was 10%, the risk (chance) of not having complications in this group was 90%. The risk of complications in the maxillary palatal fixed retainer test group was 47% and the chance of not having complications in this group was 53%. The absolute risk reduction which is the difference in risk between the test and control groups is calculated by subtracting 53% from 90% which equals a 37% reduction in risk.
Discussion
The study data suggest that there is nearly a 5-fold greater risk of complications when using a maxillary palatal fixed retainer versus a maxillary labial fixed retainer. It is much easier from a technique sensitivity perspective for clinicians to place fixed retainers on the labial surfaces of the maxillary incisors. There will be less of a chance that the dental hygienist will notice inadequate oral hygiene during periodic recall examinations. The patient can also be held responsible for not reporting any breakage when they can easily see the retainer by in the bathroom mirror. From a clinical efficiency standpoint, it was found that the time required for placement of the maxillary labial fixed retainers was much shorter in comparison to placement of the traditional maxillary palatal fixed retainer. In conclusion, the use of the maxillary labial fixed retainer has less risk of complications than the traditional palatal fixed retainer, increases productivity while lowering rework, and makes the clinicians life much easier.
The authors further postulate that orthodontists who are serious about rendering excellent treatment will rapidly adopt the labial maxillary bonded retainer. Consequently, patients will recognize the quality of care and thus the labial maxillary bonded retainer will become a status symbol in the community and a sign that the wearer cared enough to choose the best orthodontist.
References
- Ackerman MB, Thornton B. Posttreatment compliance with removable maxillary retention in a teenage population: A short-term randomized clinical trial. Ortho 2011;12:22–27.
- Zachrisson BU. Clinical experience with direct-bonded orthodontic retainers. Am J Orthod 1977;71:440-8.
- Schneider E, Ruf S. Upper bonded retainers: Survival and failure rates. Angle Orthod 2011;81:1050-1056.
Table 1: 2×2 table
| Maxillary Labial Fixed Retainer (Intervention) | |||
| Complications | Yes | No | Total |
| Yes | 3 | 14 | 17 |
| No | 27 | 16 | 43 |
| Total | 30 | 30 | 60 |
Figure 1: The budget maxillary labial fixed retainer, flat steel wire and dark adhesive.

Figure 2: The esthetic maxillary labial fixed retainer, tooth colored material and adhesive.
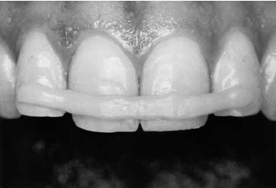
Figure 3: The noble metal maxillary labial fixed retainer, gold with labial windows and the use of clear adhesive.

Figure 4: The Custom Styled maxillary labial fixed retainer, robot bent wire and laser welded custom pads.

Figure 5: The standard maxillary palatal fixed retainer.

*The Authors have no conflict of interest in this study. They are not paid to use any of the products described herein.
Love it!
Lol – brilliant. Next step is to have resident get the data on patient satisfaction between options! Boom, another masters thesis done!
Well, well, well! As they say: “every rose as its thorn”. Standard maxillary palatal fixed retainers have forever been the worst pain in the a.. for the orthodontist. I’ve been practicing for 29 years now, and those lingual wires must account for 90% of my clinical emergencies. Now, although the idea is interesting, it will definitely call for a HUGE paradigm shift on behalf of our patients to accept the labial fixed retainer. But then again, we always thought orthodontists would never adhere to plastic for straightening teeth…Why couldn’t the patients changed on that matter in the long run.
Interesting article, but the reality is that patients will not readily accept the esthetics of a labial fixed retainer. Secondly and more significantly, by placing a fixed retainer instead of a removable one, we accept responsibility for retaining the result. We send the message to our patients that if the teeth move, it’s our fault. At some point the patients need to take that responsibility, not us.
LOL, they would love it in gold!
This article is fictitious. Samuel Clemens and Jonathan Swift were two of the greatest satirists of all time. Ackerman and I don’t claim to be in their league but it seems that we were able to produce the desired effect since so many believe this to be a serious research article. This article is wholly fabricated and is a hoax meant to point out that we orthodontists often do things that are convenient for us and effective but that patients don’t like. Stupid things like putting braces on people who want Invisalign or demanding that patients keep their appliances on even though the patient is happy and wants them off. The secondary purpose of this “article” was to encourage all of you to read and consider all the research you’re presented very carefully. Don’t believe what anyone tells you (especially us) without thinking and considering it for yourself. We don’t want to tell you what to do, we want to make you think. You’re smart people. Use your heads!