Deader than dead. As dead as the once revered science of Phrenology. I’ve suspected as much for a long time but recently, undeniable proof has surfaced in the form of a Facebook poll of all things. This question was posed to over 1400 orthodontists and orthodontic residents in Ortho101:
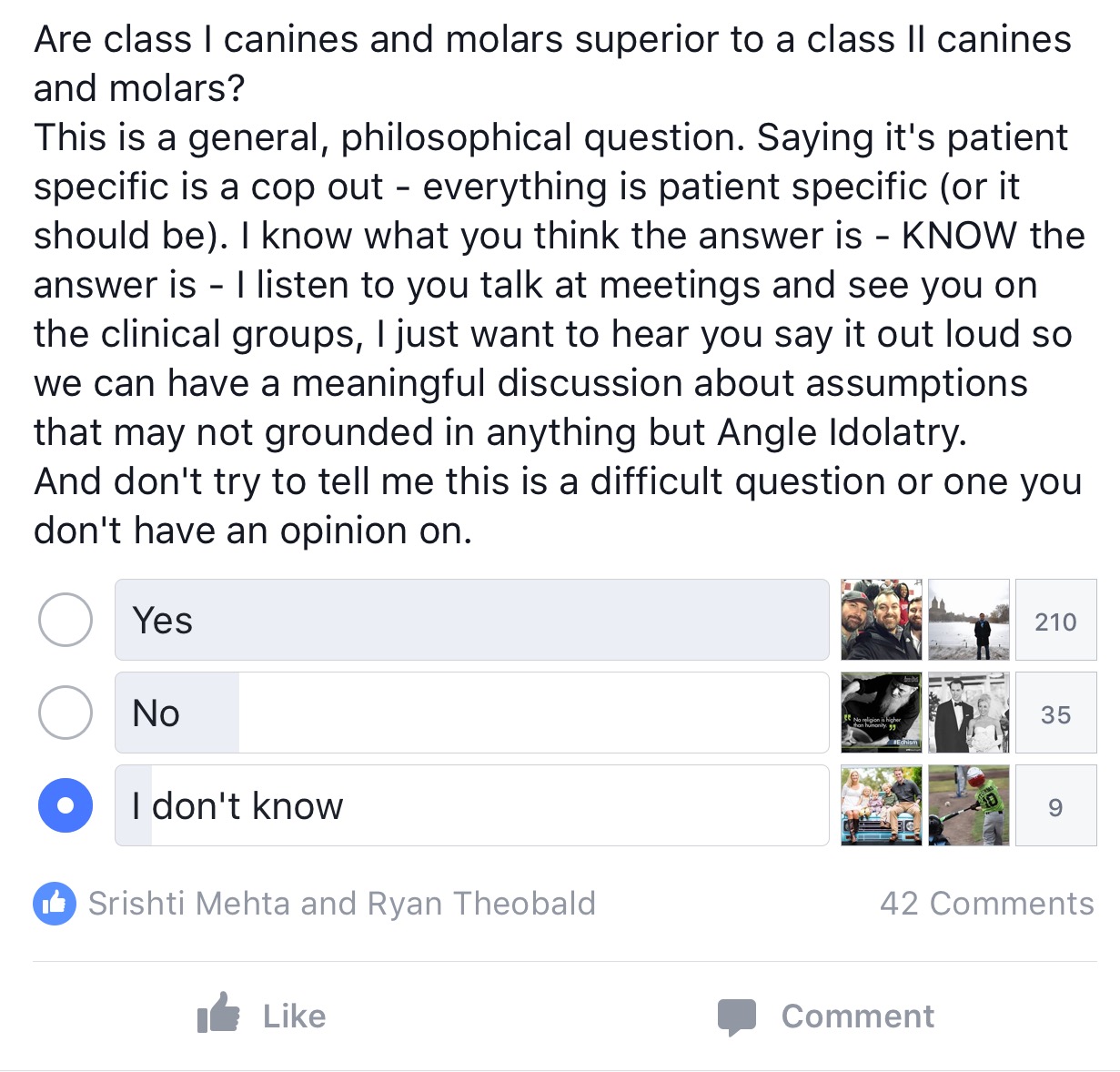
As the results clearly show, the vast majority of orthodontists and residents believe that Class I is superior to Class II occlusion – as expected. The fun began when the question “why?” was asked. No one has a good reason. No one can point to a study that says it is so. No one can come up with a single sequelae of a Class II occlusion that is unique to a Class II occlusion other than being defined as Class II! Honestly I expected a more definitive and vigorous defense of the Angle Classification System but the event itself was anticlimactic. It turns out that Angle classification IS a randomly assigned grouping of various states of occlusion based on criteria verging on irrelevance. It’s power and authority come from it’s lineage and being first… and nothing else. No? Well I’d love to hear your reasoning as to why this is inaccurate.
“What about traumatic occlusion?” I’m glad you asked. We did a Facebook poll on that as well. See for yourself:
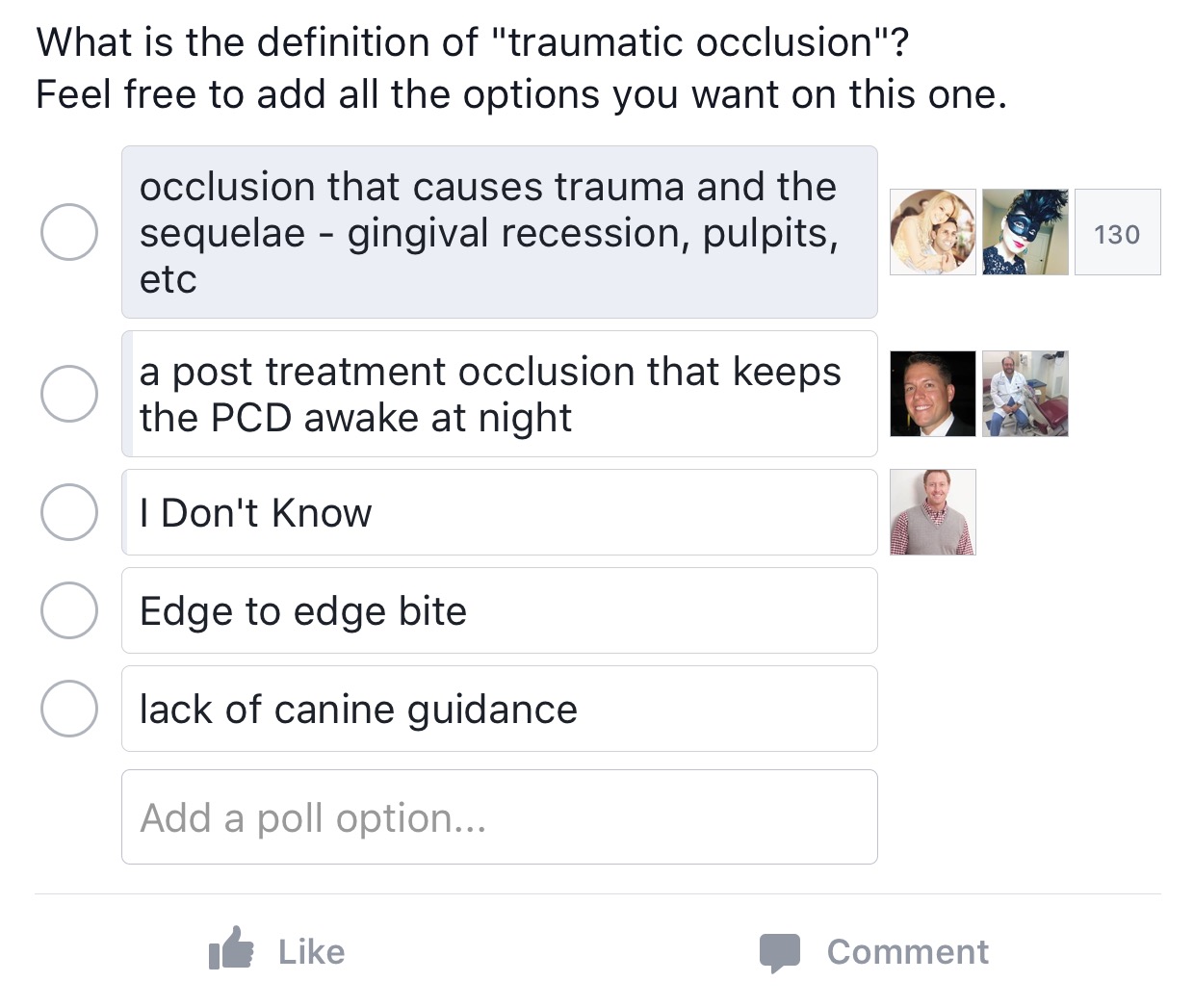
It would appear that traumatic occlusion cannot be defined by any known metric other than the detection of trauma resulting from said occlusion. This, combined with the fact that traumatic occlusion can occur as a result of all three Angle Classifications supports the premise that the Angle system is irrelevant.
“What about aesthetics? Class II cases with overjet are terrible and Div 2 cases are even worse. Class III is just plain unsightly.” I hear you saying. Ok, well, maybe to a bunch of tooth nerds like us this is true but you might want to turn on the Olympics and check out all the Class III superstars or pick up a magazine with Drew Barrymore, Rene Russo or the myriad of other Class II famous/beautiful people to see that orthodontists’ assessments of beauty doesn’t necessarily line up with that of society. The standards of beauty have changed dramatically and what is defined as beautiful is far more inclusive today. The change continues and the speed at which society’s definition of beauty changes is increasing. We orthodontists need to get our heads up and realize that our assessment of what is beautiful is not the only one (and is likely not even relevant in most cases). Maybe it’s because we are nerds and think of beauty as buccal photos with cheek retractors showing a socked in occlusion? Patient’s don’t wear cheek retractors around town…
“What about incisor guidance? Isn’t minimal overjet and overbite and canine/incisor guidance ideal? Shouldn’t that be the goal?” This is a big part of the “Class I is superior” mindset and to me, as an orthodontist, this position sounds and looks good. But there is no proof that this is the case as far as I know or that anyone can show me. So we are right back where we started.
Look, we are in a specialty that renders cosmetic, elective treatment in the vast majority of cases. We are directed by patient desires more and more every day – as it should be. Times have changed, the paternal model is dead, people are very anti-extraction, anti-discomfort, anti-compliance, anti-surgery and anti-time being spent on treatment. And all this is fine. It is the patient’s body after all and we are the hired help. What does this make us? It makes us much more akin to a sommelier than a medical doctor. We have very specific knowledge and experience and we are paid to advise the client as to the best course of action but ultimately it is the client who decides. And we, as a specialty, need to come to grips with this fact. Does this mean that we should abandon our pursuit of “ideal” overjet, overbite and a Class I occlusion? Not at all. It does mean that we should consider what it will take in terms of time and discomfort and money to get from where the patient is to where we believe they should be and that these factors should play a role in what treatment is prescribed. It also means that the patient should be informed and be part of the process, if not directing it. It means that we orthodontists should stop thinking in terms of “ideal or nothing” and realize that there is not a thing wrong with aligning the teeth of a Class II or Class III patient who doesn’t want to address the underlying skeletal issue. It won’t hurt them or you.
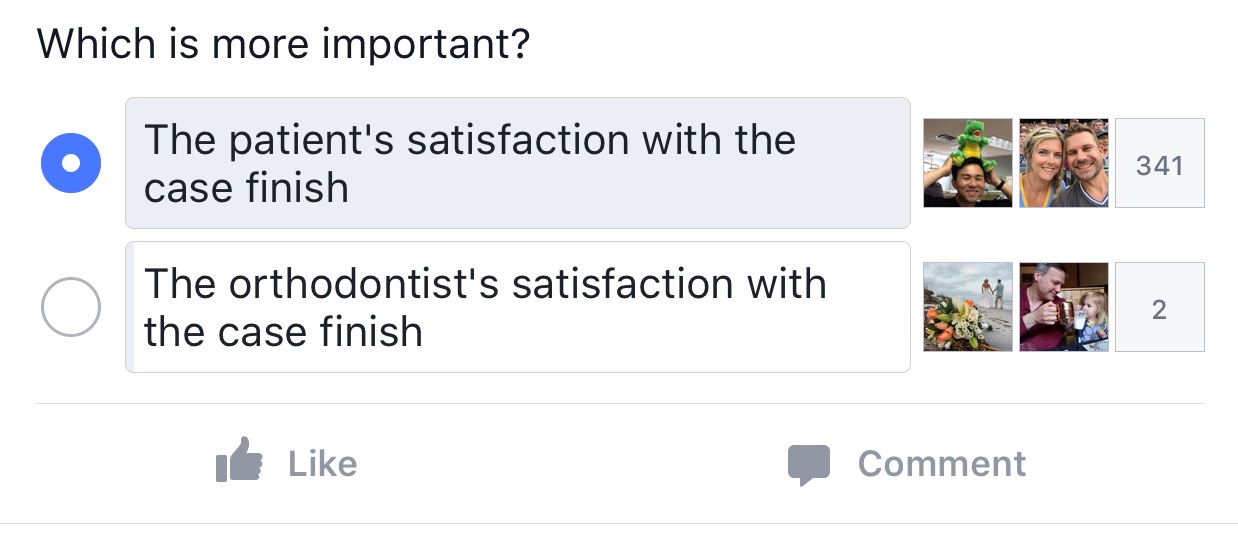
By the way, it’s not about us!
I’ll leave you with one final poll from Ortho101. Think about what this means and how the juxtaposition of this with all of the above proves the point of this entire piece. This series of polls has really made an impression on me and Marc Ackerman and now that we can plainly see proof of the truth of the matter, we plan to reassess the way orthodontists have “always done it” and see if we can come up with a more logical and relevant paradigm to supplant our specialty’s Angle Idolatry.