
By Marc Bernard Ackerman, DMD, MBA
I am the last person that you would expect to hear breaking orthodontic news from. In fact, if I am the first person to hear about something, it probably isn’t that important or if it is I’m not smart enough to realize why. So when I do get a tip, kinda like the guy on CNBC who tells you what stocks to pick, I’m pretty sure that it would have been really helpful at least a year ago! All kidding aside, as I sat in the audience at the MKS 2016 meeting this past weekend and was given the tip regarding the proliferation of the dental service organizations (DSO) venturing into orthodontics and its potential impact, I couldn’t help but think that if I was getting an “early” warning, the ship may have already set sail.
I want to share with you some of the orthodontic “tips” that I have gotten in the past two decades, present some new “tips”, er um I mean guesses (read with caution), mix ‘em up with some Kool-AidTM, serve you a tall drink and ask what it means for us now and in the future.
- Old Tip: Orthodontic residency programs will open outside of dental schools or hospitals and be linked to dental service organizations (Version 1)
- Old Tip: Too many orthodontists will graduate each year
- Old Tip: Orthodontic graduates will be laden with debt and will have to work for primary care dentists and pediatric dentists on a per diem basis (Version 1)
- Old Tip: Primary care dentists doing InvisalignTM will eat away at our patient base (Version 1)
- Old Tip: The American Board of Orthodontics will allow orthodontists to purchase initial certification, will permanently grow the numbers of diplomates, give this credential more clout and will help orthodontists get more patients
- Old Tip: Consumers will not be able to tell the difference between dentists and orthodontists and the American Association of Orthodontists should advertise that orthodontists have extra degrees (Version 1)
- Old Tip: Do it yourself orthodontics (e.g.-Smile Direct ClubTM) will eat away at our patient base (Version 2)
- Old Tip: Orthodontic graduates laden with debt will have to work for dental service organizations (Version 2)
- Old Tip: For profit CODA accredited orthodontic residency programs will open outside of dental schools or hospitals and these new schools will be owned and/or financially linked to dental service organizations (Version 2)
- Old Tip: The American Dental Association will approve Resolution 65, stating that general dentists can announce specialization and specialists can practice outside their specialty
- New Tip: For profit CODA non-accredited orthodontic residency programs will open outside of dental schools or hospitals and these new schools will be owned and/or financially linked to dental service organizations (Version 3)
- New Tip: Consumers will pay anyone who can modify their dentofacial appearance (Smile) in an efficient, effective and cost-competitive way
- New Tip: Brand-centered practices and doctor-centered practices will equally feel the changes in consumer demographics and economics in the future
- New Tip: Orthodontists will realize that AAO membership and ABO dues are better spent on local market brand/practice promotion and reinvestment in their own enterprise
- New Tip: Orthodontists will continue to whine, do the same things and wonder why they weren’t given better tips…earlier
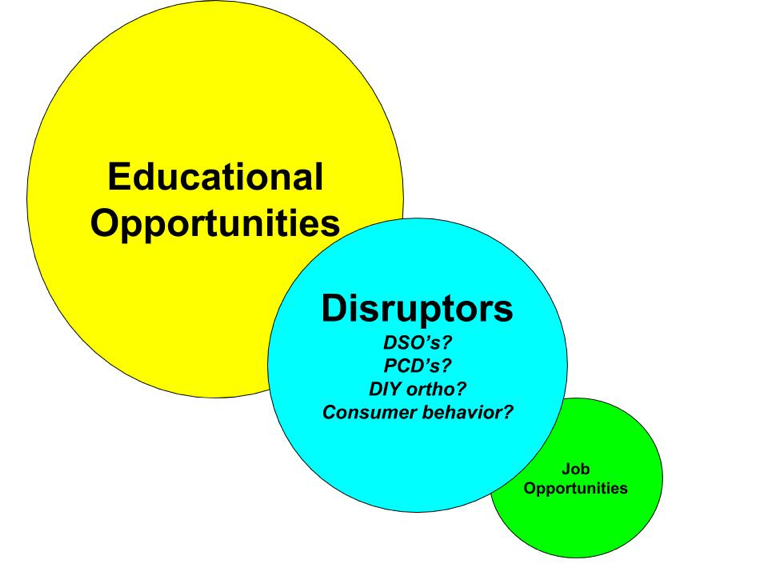
So, if you were able to read all these tips and I hope that you’re still interested, what are we to make of them? I racked my brain and have tried to find a common thread between those tips old and new. Here’s what I came up with. No one tip realized or not can account for where we are today and where we go in the future. They are all interrelated and self-perpetuated. Pictures are always better than words when it comes to presenting a theory, so here’s mine:

He who holds the educational opportunities and the jobs, controls the future. You tell me who it will be!
thank you for the tips and agree on many points. What CODA stands for? could you be more specific? thank you
also, why GP without any “officially recognized” specialty training could not do ortho and work as “orthodontists” in DSOs? After all, in EU majority of “specialty” work is done by “your friendly” GP.
Marc will be able to answer better but I can tell you that CODA is the body that gives accreditation to dental and specialty schools. I think it stands for Committee on Dental Accreditation.
Commission on Dental Accreditation
Basically it is an arm of the ADA, but I am not sure of the entire nature of this entangled alliance. They are responsible for accrediting dental schools, dental specialties, gprs, and fellowships in dental areas.
At this point it is pretty much a rubber stamp. Having participated as a faculty member in several orthodontics programs that underwent site visits, its a bit of a joke. The program has to answer a sequence of detailed questions in written form and send the responses to CODA prior to the site visit. It usually takes a few 4 inch binders to satisfy them. I also believe that site visitors are chosen from academic programs that are not from the program’s geographic area. I can’t remember if you can ask that a certain person be excluded (it has been over 5 years since my last one). The visitors come in and tour the facility. They talk to the Chair, Faculty, and residents. They also may talk to the Dean or Associate Dean for finance to assess the financial support/viability of the program.
The site visitors leave and then prepare a formal report to the commission. They can suggest full accreditation, accreditation with reporting requirements (that’s like remediation in some area is needed) or they can recommend removal of accreditation. In orthodontics, I don’t believe that any program in the past 20 years has lost accreditation.
This is what actually happens. The old binders from 7 years prior (the last accreditation cycle) are updated by changing dates and faculty names and other minor variations. The faculty meet. The chair talks about what to say and what not to say. The residents are told to keep their mouths shut. The visitors will come and the chair will usually be buddies with at least one of the visitors. The visit comes off without a hitch and then the rubber stamp is applied.
This is why so many new programs are able to open. The precedent of accrediting the first orthodontic program without being related to a dental school or hospital occured without a pre-emptive fight from the AAO. Now since so many have been opened, they would be exposed to great legal distress if they tried to interfere.
Dr. Ackerman, simply, thank you for this post. You just summed up the future of orthodontics in a couple of paragraphs. My recommendation is for you to run for AAO president because you have the foresight to see what’s really going on and can save our specialty. If you decide to run let me know so I can support you in any way I can. Or perhaps we can start something grassroots independent of them so we don’t have to jump through administrative hoops to make a real difference.
Intellectual propriety is what we have. The problem is that there’s too many of us. They only other sentiment I would add here is that to thrive and be profitable and bust, we need to be the “orthodontists orthodontist” or a “super-orthodontist” which means having the ability to be efficient at diagnosing and treating the challenging cases and repair jobs that the PCD’s mess up or have the sense not to touch. That, and treating the “crazies”. Similar to what’s going on in prosthodontics. Except there’s a lot less of them. Thanks again for the insight.