

Marc Bernard Ackerman, DMD, MBA
Orthodontists cannot modify growth of the craniofacial skeleton. Orthodontists can sort of identify patterns of craniofacial growth but we are mediocre predictors of its timing and extent. Most studies using longitudinal cephalometric methods are pseudoscience at best. Yet contemporary orthodontists are the proud beneficiaries of the radiographic and plaster cast data from 9 of the original 12 craniofacial growth studies that were conducted in the first three quarters of the 20th century. AAOF fundraising has preserved and digitally made available all of the material that survives from these studies. This Herculean task must have been daunting for the academic participants and must have consumed many hours away from other activities perhaps even clinical practice.
How should we view this material in the modern world? Well, there is an ethical answer and a relevance answer. Ethically, this type of research with ionizing radiation administered in greater frequency than intended would never be approved by a University or Contract Research Organization’s institutional review boards (IRB) and we shouldn’t be too proud of our forebear’s misdeeds. In terms of relevance, the role of cephalometric and growth analysis in the treatment of today’s orthodontic patient is in the rearview mirror. Orthodontic diagnosis via clinical evaluation of the face/smile and the assessment of three-dimensional models of the dentition account for at least 90% of treatment decisions.
Pre and post treatment cephalometric analysis is nothing more than a feel good exercise for orthodontists who wish to measure how far they moved the teeth vertically and anteroposteriorly. Since there is no prognostic or therapeutic value to the post treatment cephalometric film except what some orthodontists would call a “treatment post-mortem”, why do we still take it? Simple, the American Board of Orthodontists requires it. The British Orthodontic Society has published comprehensive guidelines for the use of radiographs in clinical orthodontic practice. Here are their conclusions captured from page 27 of the report:
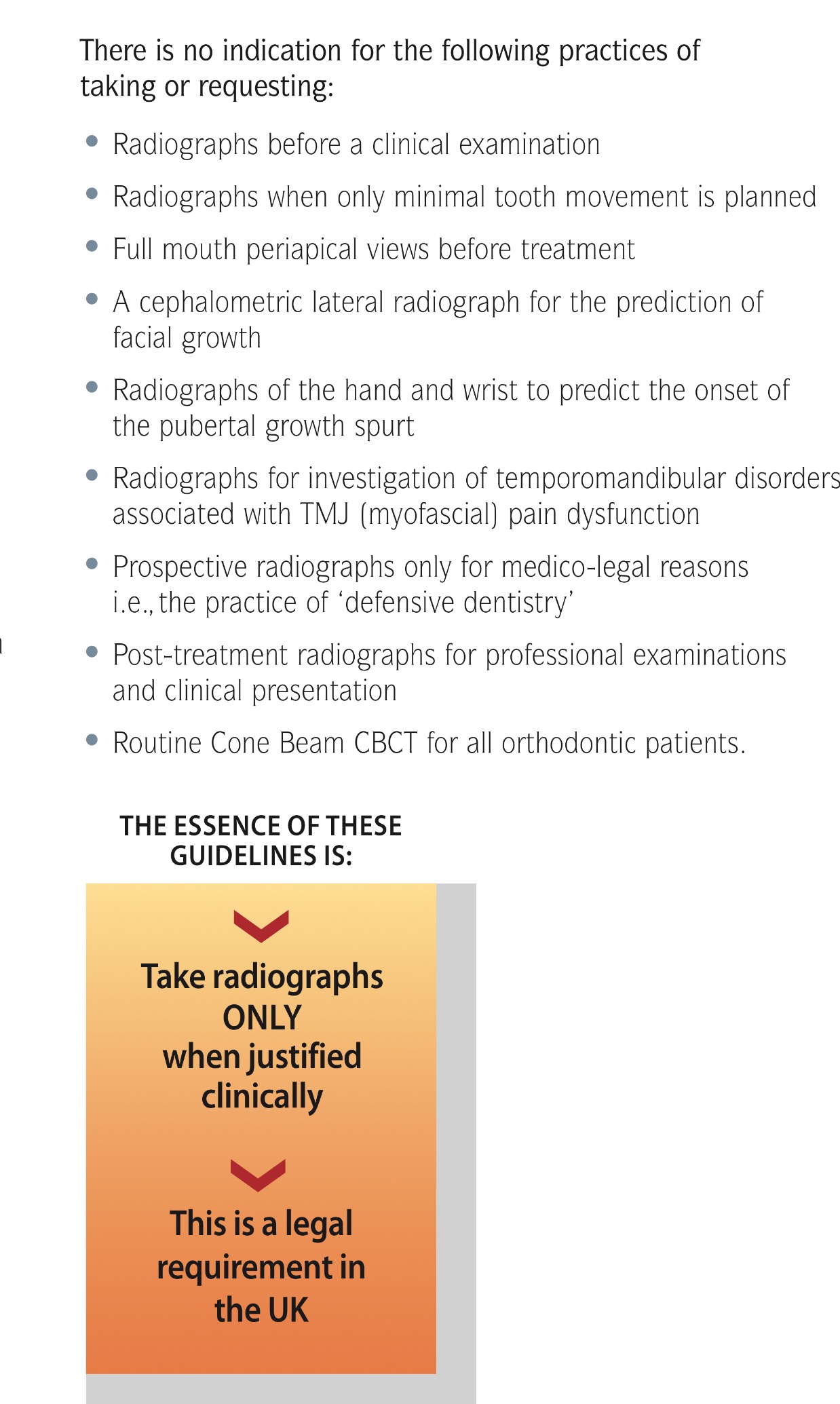
Can someone please tell me why American orthodontists and in particular the American Board of Orthodontics are so reticent to talk about taming our addiction to exposing patients to unnecessary ionizing radiation (cephs and CBCTs)? Is it ethically justifiable to expose patients to these radiographs when the threshold dose that carries the risk of cancer induction is unknown? I hate to say it but the British are winning the revolutionary war of common sense!
Common sense!
Exactly. Not so common unfortunately!