

I had a very interesting conversation with a dental school classmate today. He’s one of the smartest people I know and given his class rank in dental school, he could have done any specialty he wanted. In general practice now, he was asking me the best way to communicate to an orthodontist the minimum space he needed for an implant replacing a lateral. Here’s a transcript of the messenger convo:
Classmate: Question for the ortho expert. I’ve gotten a few cong missing laterals post ortho with 5 mm or less space, almost making implants impossible. I’d like to make a visual for ortho when I refer these cases. What do you think of minimum space specs and honestly speaking is this difficult to accomplish for orthodontists?
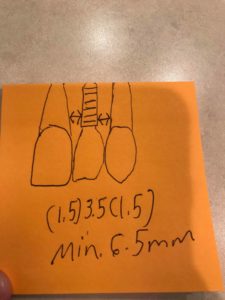
Ben: It’s problematic for several reasons. First unless they are using 3D X-ray it’s impossible to get a real measurement from a pano. Second if you have locked in class I canines and the midline is on and they have minimal overjet and overbite then there’s really no more room unless you want excess overjet. Honestly in missing lateral cases I’m much more in favor of closing the missing lateral space and reshaping the canines unless the patient has a class III skeleton. The AJODO released a study last year that shows that laypersons couldn’t tell the difference. Plus even if an implant and crown look great now they won’t in 20 years. Anterior implants all show eventually and look bad in my experience. This position has not endeared me to formerly referring dentists as you might guess but canine substitution is what I would do for my kids or my wife if they were missing a lateral. Call me if you want to discuss. This is a big topic with lots of details. xxx-xxx-xxxx is my cell.
Classmate: Not to mention the facial to lingual bone is usually highly resorbed in this area, also posing a huge challenge. I’ll def give ya a call later as this issue is just really sucky from all angles.
Ben: Canine substitution is almost always a great option as long as they don’t have an underbite. Funny we are discussing this now. I just had a class III kid with missing upper laterals come in for a NP visit. It’s an implant case all the way. I referred him to another orthodontist because those cases are a nightmare given the lack of effective communication between orthos and general dentists!
Classmate: Bingo. All about communication cause everyone wants case to be a success, but complicates everything without communication. Just had one with 7 missing and 10 a peg. Interesting that Carl misch the granddaddy of implants liked to remove primary laterals early allowing canines to drop in, bringing bone with it. Then later, moving canines back into normal slots with implants. He stated this resulted in ample bone. But I bet that’s a bear for ortho to achieve.
Ben: It’s a bear to move teeth posteriorly for sure. the idea of distalization is mostly a myth. If I see a kid young (that’s my preference) I’ll try to get the canines to erupt into the missing lateral space so it is easier to reshape and substitute. I’ve done hundreds of substation cases. they look good when they are first done but compared to a 20 year old implant they look frigging awesome. It’s a long game from where I sit.
Classmate: Ya. Great points I hadn’t considered. It’s also increasingly an issue (at least we’re aware of it now) that continued growth through life will certainly affect Incisal heights of implants as they are ankylosed. Even in implants placed long after “growth” is complete. Heck, even if someone were extremely cosmetically picky conservative veneers on 5,6,11, and 12 would be cosmetically superior to implants long term and likely short term. Long term buccal plate loss with “graying” of gingiva is common as well with the lateral implants.
Ben: Exactly!
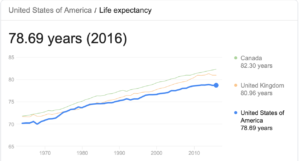
I sure wish every discussion I’ve had with a general dentist (or other orthodontists for that matter) had gone half this well. My classmate is correct that most if not all of us want to get a good result but in these implant prep cases for missing laterals the general dentists become annoyed because orthodontists can’t always deliver the minimum space they need and the orthodontists get frustrated because they try to explain why the space is what it is in many cases. Communication is the key but honestly gang, there is very little to suggest that doing anterior implants instead of closing missing tooth space is the way to go except in cases where the skeletal relationship precludes doing so. No matter how good an implant looks at the time it is placed or how bad you think a reshaped canine will look, give it 20 years and I guarantee the canine substation case will look much better. Given the average lifespan these days, don’t we owe it to our patients to think long term?
Not to mention that the cost of a single implant and crown rivals the cost of orthodontics PLUS implants will likely have to be redone a couple times over the patient’s lifetime.